
You noticed blood — but your period isn’t due for another two weeks. Or maybe it ended just days ago and you’re spotting again. It’s unsettling, and your mind immediately goes to the worst-case scenarios. Now with the help of period calculator we can easily check our next period date.
Here’s the truth: bleeding between periods, medically called intermenstrual bleeding or abnormal uterine bleeding (AUB), affects roughly 14–25% of women of reproductive age at some point in their lives. Sometimes it means almost nothing. Other times, it’s your body’s way of signaling something that genuinely needs attention.
This guide covers every clinically recognized cause of menstrual bleeding between periods — not just the five or six causes that most articles recycle. We’ll explain what each condition looks and feels like, how it’s diagnosed, what makes it better, and — critically — when you should stop waiting and call your doctor today.
What Counts as “Bleeding Between Periods”?
Before diving into causes, it’s worth defining what we’re talking about — because the terminology varies and can cause confusion.
A normal menstrual cycle lasts between 21 and 35 days, with bleeding that typically lasts 3–7 days. Anything that falls outside this pattern may be considered abnormal.
Bleeding between periods can look like:
- Light spotting — just a few drops of pink or brown discharge
- Heavier breakthrough bleeding — enough to require a pad or tampon
- Post-coital bleeding — bleeding after sexual intercourse
- Mid-cycle bleeding — occurring around ovulation
- Irregular staining — unpredictable, with no clear pattern
The color, amount, timing, and associated symptoms all matter. A single episode of light pink spotting mid-cycle is clinically very different from recurring heavy bleeding two weeks after your period ends.
The Full Spectrum: 15 Causes of Menstrual Bleeding Between Periods
1. Hormonal Imbalance
The most common single category behind abnormal intermenstrual bleeding is a disruption in the hormonal orchestra that controls your cycle — specifically the balance between estrogen and progesterone.
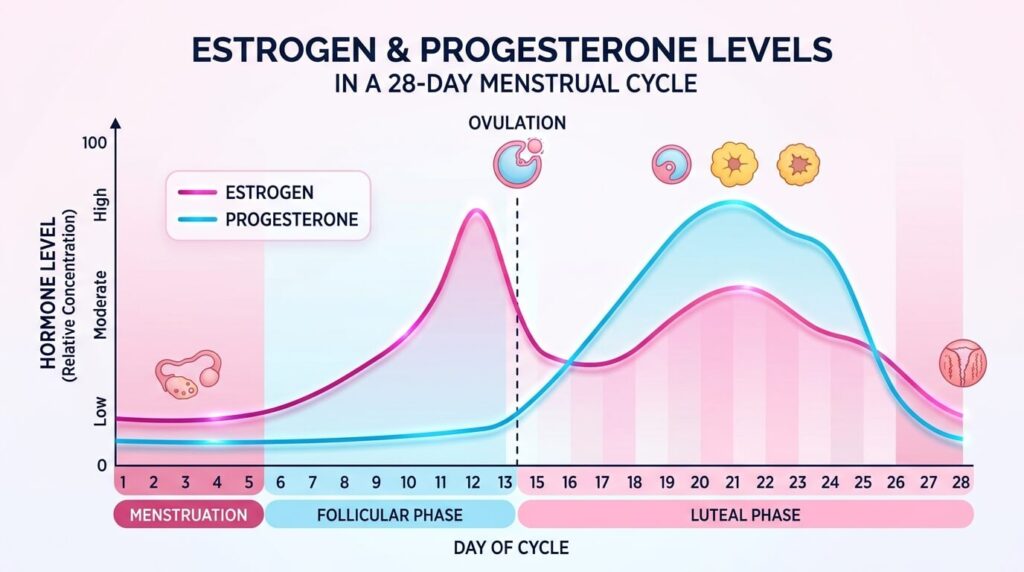
Your menstrual cycle runs on a tightly timed sequence. Estrogen rises in the first half of the cycle to thicken the uterine lining. After ovulation, progesterone takes over to stabilize that lining. If either hormone dips or surges at the wrong time, the lining can shed unpredictably, causing breakthrough bleeding.
Who experiences this most? Teenagers whose cycles haven’t yet regulated, women in their 40s approaching perimenopause, and anyone under significant physical or emotional stress.
What it looks like: Light-to-moderate spotting, often not tied to any particular day of the cycle. It may happen every month or be completely random.
2. Birth Control and Hormonal Contraceptives
Hormonal contraception is one of the most frequent causes of spotting between periods — and it’s one of the most under-explained.
The pill: During the first 3 months of starting or switching a combined oral contraceptive pill, breakthrough bleeding is extremely common. The synthetic hormones are essentially “teaching” your uterus a new pattern. Missing even a single pill can trigger spotting.
Progestin-only methods (mini-pill, hormonal IUDs, implants, injections): These are particularly associated with unpredictable spotting, especially in the first 6 months. Progestin-only formulations thin the uterine lining, which can cause it to shed at irregular intervals.
Intrauterine devices (IUDs): Both hormonal and copper IUDs can cause spotting, particularly in the first 3–6 months after insertion. The copper IUD (non-hormonal) may also make periods heavier and longer.
Emergency contraception (“morning-after pill”): A high dose of hormones can disrupt the current cycle, causing bleeding within days of taking it.
Practical tip: If you’ve started new hormonal contraception within the last 3 months, breakthrough spotting is probably an adjustment response, not a symptom of a new problem. But if it persists beyond 3 months or is heavy enough to soak a pad, contact your prescriber.
3. Ovulation Bleeding (Mittelschmerz)
Around the middle of your cycle — typically around day 14 in a 28-day cycle — your ovary releases an egg. This process causes a brief, sharp drop in estrogen just before the surge that triggers ovulation.
For some women, this hormonal dip causes light spotting for 1–2 days. This is called ovulation bleeding or, if accompanied by pelvic pain, Mittelschmerz (German for “middle pain”).
Characteristics:
- Timing: consistently around the midpoint of your cycle
- Amount: very light — more of a pink or brownish tinge than actual flow
- Duration: 1–3 days at most
- Other signs: mild one-sided pelvic cramping or ache, increased cervical mucus
Is it dangerous? Not at all. Ovulation bleeding is a normal physiological variation. However, it should be consistently mid-cycle and mild. If the pattern changes, have it evaluated.
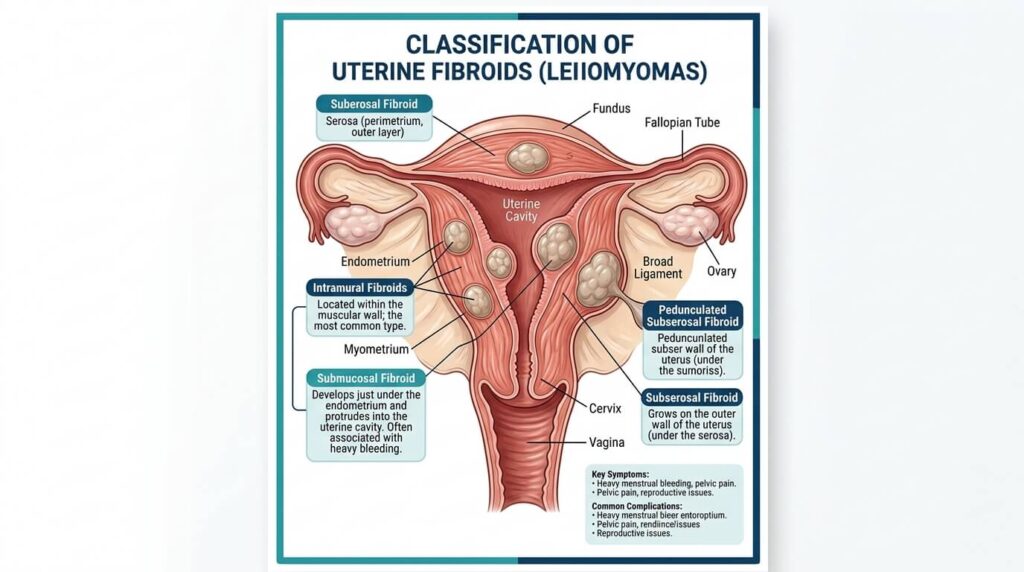
4. Uterine Fibroids
Uterine fibroids — noncancerous growths of muscle tissue in or around the uterus — affect an estimated 70–80% of women by age 50, though many never cause symptoms. When they do, abnormal bleeding is often the first and most prominent complaint.
The location of a fibroid matters more than its size. Submucosal fibroids (those that grow into the uterine cavity) are most likely to cause heavy bleeding, including between periods, because they directly disrupt the uterine lining. Intramural fibroids (within the muscle wall) can also cause irregular bleeding when they’re large enough.
Other symptoms to watch for:
- Pelvic pressure or a sensation of fullness
- Frequent urination
- Constipation or rectal pressure
- Back or leg pain
- Prolonged, heavy periods with clots
Fibroids are diagnosed via ultrasound, and treatment ranges from watchful waiting (if symptoms are mild) to medications, non-surgical procedures like uterine fibroid embolization, or surgery.
5. Uterine Polyps
Uterine polyps are soft, finger-like growths that develop from the endometrium (uterine lining) and project into the uterine cavity. They’re usually benign, but they can cause significant irregular bleeding — including spotting between periods, heavy periods, and bleeding after menopause.
Unlike fibroids, polyps are soft and often smaller. They’re more common in women aged 40–50, though they can appear at any age. They’re often discovered incidentally during an ultrasound ordered for something else.
Why they bleed: Polyps have their own blood supply and fragile surface tissue. When compressed or when their blood supply is compromised, they bleed erratically.
Diagnosis: Transvaginal ultrasound can suggest polyps, but hysteroscopy (a thin camera inserted through the cervix) is the gold standard. Most polyps can be removed during the same hysteroscopic procedure.
One thing competitors miss: A small percentage of uterine polyps — particularly in postmenopausal women — can harbor precancerous or cancerous cells. This is why evaluation matters even when polyps seem “minor.”
6. Endometriosis
Endometriosis occurs when tissue resembling the uterine lining grows outside the uterus — on ovaries, fallopian tubes, pelvic sidewall, bladder, or bowel. This misplaced tissue responds to hormonal signals just like the uterine lining does: it thickens, breaks down, and bleeds with each cycle — but has nowhere to go.
This internal bleeding causes inflammation, scarring, and adhesions. It also causes irregular bleeding that may appear as spotting between periods, especially in the days leading up to menstruation.
The hallmarks of endometriosis:
- Severe, progressively worsening menstrual cramps
- Pain during sex (dyspareunia)
- Painful bowel movements or urination during menstruation
- Chronic pelvic pain
- Difficulty conceiving
Endometriosis affects roughly 10% of women of reproductive age globally and is notoriously underdiagnosed — with an average delay of 7–10 years from symptom onset to diagnosis.
Diagnosis requires laparoscopy (minimally invasive surgery) for definitive confirmation, though MRI and ultrasound can suggest severe disease. Treatment includes hormonal therapies and surgical removal of endometrial implants.
7. Polycystic Ovary Syndrome (PCOS)
PCOS is a hormonal disorder affecting an estimated 8–13% of reproductive-age women. It disrupts normal ovulation, leading to irregular or absent periods — and, paradoxically, to unexpected bleeding when the uterine lining finally sheds after a long buildup.
Women with PCOS often have elevated androgens (male hormones), multiple small follicles on the ovaries (visible on ultrasound), and irregular menstrual cycles that can range from very frequent to very infrequent.
What causes the between-period bleeding in PCOS? When ovulation is suppressed for weeks or months, estrogen continues to build up the uterine lining without the progesterone surge that should follow ovulation. Eventually, the unstable lining sheds in an unpredictable, often heavy pattern.
Other PCOS symptoms include excess facial or body hair, acne, hair thinning, weight gain concentrated around the abdomen, and skin darkening in body creases.
8. Thyroid Disorders
The thyroid gland — a butterfly-shaped organ in your neck — produces hormones that regulate metabolism, body temperature, and yes, your menstrual cycle.
Hypothyroidism (underactive thyroid): Low thyroid hormone levels can cause heavier, more frequent periods or irregular bleeding between cycles.
Hyperthyroidism (overactive thyroid): Excess thyroid hormones can lead to lighter, less frequent periods — but may also cause unpredictable spotting.
This connection is frequently overlooked by women and even some clinicians. If you have irregular bleeding alongside symptoms like fatigue, unexplained weight changes, hair thinning, feeling cold all the time, or a racing heart, ask your doctor to check your thyroid function (TSH, T3, T4).
9. Sexually Transmitted Infections (STIs)
Chlamydia and gonorrhea — the two most common bacterial STIs — can silently infect the cervix and cause post-coital bleeding or spotting between periods. They frequently have no other symptoms at all, which is why regular STI screening is so important for sexually active women.
Pelvic inflammatory disease (PID) — an infection of the uterus, fallopian tubes, and/or ovaries, often caused by untreated chlamydia or gonorrhea — is another cause. PID typically causes pelvic pain, fever, unusual vaginal discharge, and irregular bleeding.
Trichomoniasis (a parasitic STI) and bacterial vaginosis (BV, an imbalance of vaginal bacteria) can also cause spotting or bleeding through cervical irritation.
10. Cervical Pathology: Ectropion, Polyps, and Cancer
Cervical ectropion (also called cervical erosion) occurs when the soft, glandular cells from inside the cervical canal spread to the outer surface of the cervix. This tissue is delicate and bleeds easily — most commonly after sex, but sometimes spontaneously.
It’s particularly common in women who:
- Are pregnant
- Take oral contraceptives
- Are in their teens and early 20s
Cervical ectropion is benign and often requires no treatment, though it can be treated with cryotherapy if bleeding is persistent and bothersome.
Polyps — small, benign stalked growths on the cervix — also cause spotting, especially after intercourse.
Cancer is a much rarer but critically important cause that must be excluded. Early-stage cervical cancer may have no symptoms at all, or only irregular bleeding and watery, possibly blood-tinged vaginal discharge. This is why Pap smears and HPV testing are lifesaving screening tools, not just routine box-ticking.
11. Pregnancy-Related Causes
Any time a woman of reproductive age experiences unexpected bleeding, pregnancy must be considered — even if she’s using contraception.
Implantation bleeding: When the fertilized egg embeds into the uterine wall (typically 6–12 days after conception), some women experience light spotting for 1–3 days. This is often mistaken for an early, light period.
Miscarriage: Approximately 10–20% of known pregnancies end in miscarriage, most in the first trimester. Heavy cramping and bleeding are the hallmarks, but some miscarriages begin with only light spotting.
Ectopic pregnancy: This occurs when a fertilized egg implants outside the uterus — most commonly in a fallopian tube. Ectopic pregnancies are medical emergencies. Symptoms include sharp abdominal or pelvic pain (often one-sided), vaginal bleeding, shoulder tip pain, and dizziness. If untreated, the tube can rupture.
Subchorionic hemorrhage: Blood pooling between the placenta and uterine wall, more common in the first trimester. Can cause significant bright red bleeding and is usually detected on ultrasound.
If there is any chance of pregnancy and you’re experiencing bleeding, take a home pregnancy test and seek medical care promptly.
12. Medications That Cause Abnormal Bleeding
Several commonly prescribed medications can disrupt the menstrual cycle or cause bleeding:
- Anticoagulants (blood thinners): Warfarin, heparin, rivaroxaban, apixaban — these reduce the blood’s ability to clot, which can result in heavier periods or breakthrough bleeding.
- Antipsychotics: Certain medications like risperidone raise prolactin levels, which disrupts ovulation and can cause irregular bleeding.
- Corticosteroids: Long-term use can affect hormonal balance.
- Tamoxifen: Used in breast cancer treatment; can cause irregular uterine bleeding and increases the risk of uterine polyps and endometrial cancer with long-term use.
- Herbal supplements: Ginkgo biloba, ginseng, and dong quai have anticoagulant or estrogenic properties that can affect bleeding patterns.
Always tell your gynecologist every medication and supplement you take when discussing abnormal bleeding.
13. Perimenopause
The years leading up to menopause — typically beginning in a woman’s mid-to-late 40s — are marked by fluctuating and eventually declining estrogen levels. This causes periods to become irregular, skip months, or return after an absence. Breakthrough bleeding is common and expected during perimenopause.
However, any bleeding after 12 consecutive months without a period (true menopause) is abnormal and must be investigated. Postmenopausal bleeding can indicate uterine polyps, endometrial hyperplasia, or endometrial cancer — and warrants urgent evaluation.
14. Endometrial Hyperplasia
When estrogen is not balanced by progesterone (as happens in anovulatory cycles, PCOS, or obesity), the uterine lining can overgrow — a condition called endometrial hyperplasia. This causes irregular, often heavy, breakthrough bleeding.
Simple endometrial hyperplasia without atypia is usually benign and responds to progestin therapy. However, complex atypical hyperplasia carries a meaningful risk of progressing to endometrial cancer (roughly 25–30% if untreated) and often requires hysterectomy.
This is one of the most under-discussed causes in competitor articles — and one of the most clinically significant.
15. Stress, Weight Changes, and Systemic Illness
The hypothalamus — the brain region that governs reproductive hormones — is acutely sensitive to physiological stress. Significant weight loss or gain, extreme exercise, severe psychological stress, chronic illness, or nutritional deficiencies can all disrupt the hormonal axis that controls menstruation.
Eating disorders (particularly anorexia nervosa) commonly cause amenorrhea (absent periods) or highly irregular cycles. Rapid weight gain associated with insulin resistance can drive the hormonal dysfunction seen in PCOS.
Systemic conditions like liver disease, kidney disease, and coagulation disorders (such as von Willebrand disease) can all affect menstrual bleeding patterns.
When Is Bleeding Between Periods an Emergency?
Most causes of intermenstrual bleeding are not immediately life-threatening. But some are. Seek emergency care or call emergency services immediately if you experience:
- Heavy bleeding soaking more than one pad or tampon per hour for two or more consecutive hours
- Signs of ectopic pregnancy: sharp one-sided pelvic pain, shoulder tip pain, fainting, dizziness, pale skin — especially with a positive or uncertain pregnancy test
- Signs of miscarriage with significant pain and heavy clotting
- Postmenopausal bleeding — even a small amount, even once
- Bleeding accompanied by fever, severe pelvic pain, and foul-smelling discharge (signs of PID or infection)
When to See Your Gynecologist (Non-Emergency)
Schedule a gynecologist appointment within the next 1–2 weeks if:
- Spotting occurs in three or more consecutive cycles
- Bleeding is heavy enough to disrupt daily activities
- Bleeding occurs after sex on more than one occasion
- You’re over 40 and notice any change in your bleeding pattern
- You have known risk factors for endometrial cancer (obesity, PCOS, diabetes, family history)
- You’re postmenopausal and notice any bleeding
- You have pelvic pain, pressure, or fullness alongside the bleeding
- Your current contraception seems to be causing excessive, persistent spotting
How Abnormal Uterine Bleeding Is Diagnosed
A thorough evaluation typically includes:
History and physical exam: Your doctor will ask about the timing, amount, color, and pattern of bleeding; your menstrual history; sexual activity; contraceptive use; medications; and other symptoms.
Pregnancy test: Almost always the first step in any woman of reproductive age.
Blood tests: Complete blood count (to check for anemia), hormone levels (FSH, LH, estradiol, progesterone, prolactin, thyroid function), and sometimes coagulation studies.
Pelvic ultrasound / Transvaginal ultrasound (TVUS): A highly informative, non-invasive imaging tool that can identify fibroids, polyps, ovarian cysts, endometrial thickness, and structural abnormalities.
Endometrial biopsy: A small sample of the uterine lining is taken in office and sent for pathology. Essential for ruling out endometrial hyperplasia and cancer, particularly in women over 35 with risk factors.
Hysteroscopy: A thin camera is inserted through the cervix to directly visualize the uterine cavity. The most accurate method for diagnosing polyps, fibroids within the cavity, and subtle structural problems.
Cervical cultures / STI testing: Swabs to check for chlamydia, gonorrhea, and other infections.
Pap smear and HPV test: To evaluate the cervix.
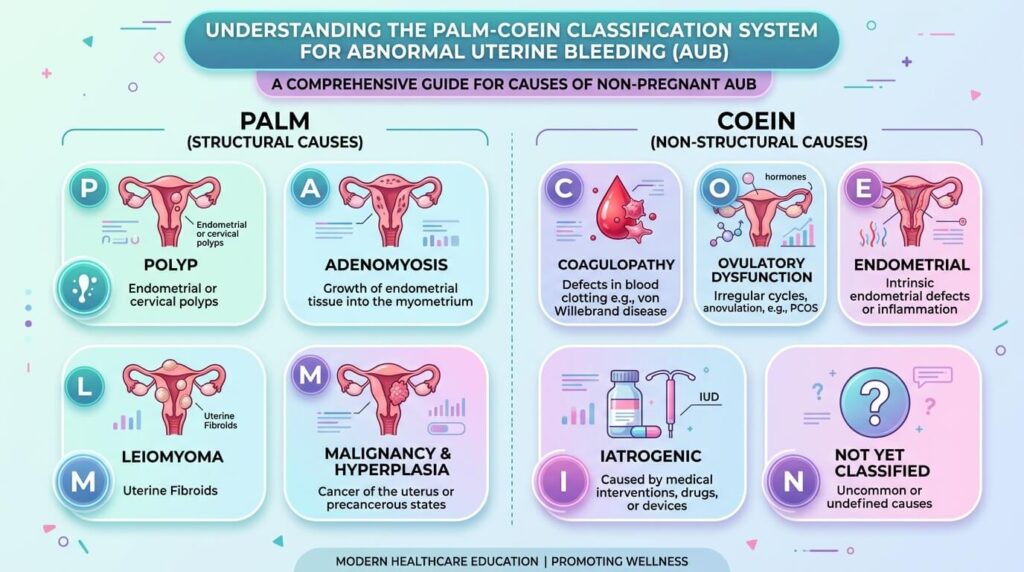
The PALM-COEIN Classification: What Your Doctor Is Thinking
When evaluating abnormal uterine bleeding, gynecologists often use the PALM-COEIN classification system developed by the International Federation of Gynecology and Obstetrics (FIGO).
| Category | Stands For |
|---|---|
| P | Polyp |
| A | Adenomyosis |
| L | Leiomyoma (fibroids) |
| M | Malignancy and hyperplasia |
| C | Coagulopathy (clotting disorders) |
| O | Ovulatory dysfunction |
| E | Endometrial dysfunction |
| I | Iatrogenic (medication/device-related) |
| N | Not yet classified |
This framework helps clinicians systematically work through every structural and functional cause of bleeding, rather than jumping to conclusions.
Treatment Options: What Actually Helps
Treatment depends entirely on the cause, but here’s an overview of the most common approaches:
Hormonal therapies:
- Combined oral contraceptive pills to regulate cycles
- Progestin therapy (oral, injectable, or IUD) to counteract excess estrogen
- GnRH agonists to temporarily suppress the cycle (used before surgery for fibroids or endometriosis)
- Hormonal IUD (Mirena) — one of the most effective treatments for heavy, irregular bleeding from multiple causes
Non-hormonal medications:
- Tranexamic acid — reduces bleeding by preventing blood clot breakdown; used for acute heavy bleeding episodes
- NSAIDs (like ibuprofen) — reduce bleeding volume and cramping
Surgical options:
- Hysteroscopic polypectomy — removal of uterine polyps
- Myomectomy — surgical removal of fibroids (preserves the uterus)
- Uterine fibroid embolization (UFE) — minimally invasive procedure cutting off blood supply to fibroids
- Endometrial ablation — destroys the uterine lining; effective for abnormal bleeding in women who don’t want future pregnancy
- Hysterectomy — removal of the uterus; definitive treatment for severe cases
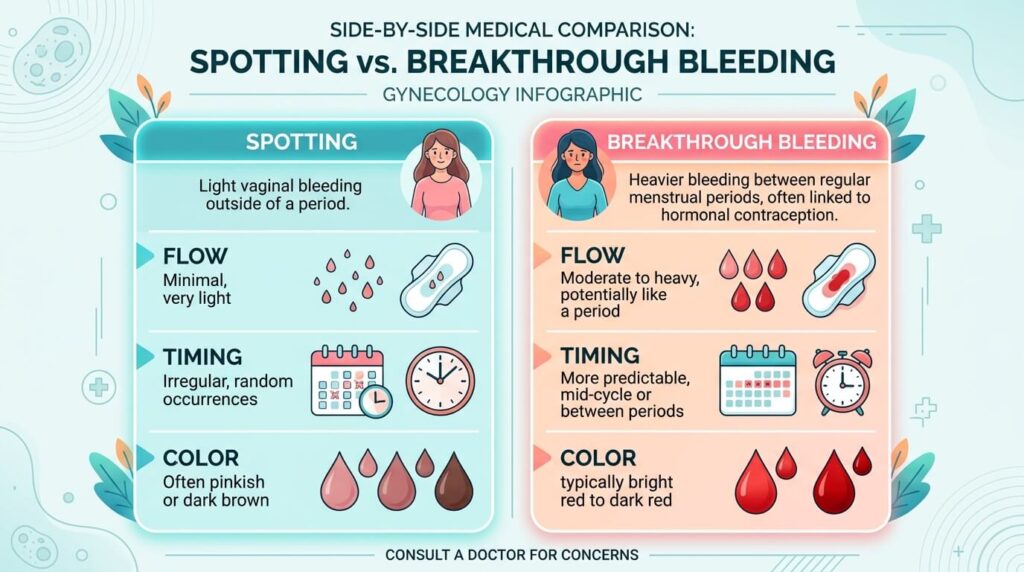
Spotting vs. Bleeding: Does the Difference Matter?
Yes. Though the terms are sometimes used interchangeably:
Spotting is very light bleeding — a few drops of blood, usually pink, brown, or rust-colored. It doesn’t fill a pad or tampon and may only be noticed when wiping.
Breakthrough bleeding or intermenstrual bleeding is more substantial — enough to require menstrual protection.
Brown or rust-colored spotting typically represents older blood that took longer to exit the body — often less urgent than bright red bleeding. But timing, frequency, and associated symptoms still matter regardless of color.
Keeping a Bleeding Journal: Practical Advice Your Doctor Will Thank You For
When you arrive at your appointment, the more specific information you can provide, the faster and more accurately you’ll be diagnosed.
Track the following for at least two cycles:
- First day and last day of each period
- Amount of flow each day (number of pads/tampons used)
- Any spotting or bleeding outside your period — the date, color, amount, and duration
- Whether bleeding occurred after sex
- Associated symptoms: cramping, pain location, discharge, fatigue
- Any medications or supplements taken
Many period-tracking apps (like Clue, Flo, or Ovia) have features for logging spotting. Or a simple notebook works fine.
Conclusion
Bleeding between periods is not something to dismiss or wait out indefinitely. While many causes — ovulation spotting, early contraceptive adjustment, minor hormonal fluctuation — are completely benign, others require prompt diagnosis and treatment.
The causes of menstrual bleeding between periods range widely: hormonal imbalances, structural issues like fibroids and polyps, conditions like PCOS, endometriosis and thyroid disease, infections, medications, and in rarer cases, cancer. Pregnancy-related causes always need to be excluded first.
The common thread is this: your body is telling you something. Whether it’s a whisper or a shout depends on context. But when bleeding consistently occurs outside your expected cycle — or when it’s accompanied by pain, fever, heavy flow, or postmenopausal timing — it deserves medical attention, not reassurance from a search engine.
See your gynecologist. Ask about the PALM-COEIN categories. Keep a bleeding journal. Get the testing done. And know that in the vast majority of cases, this is something that can be explained, treated, and resolved.
Frequently Asked Questions (FAQ)
Q: Is it normal to bleed a little between periods?
A: Light, mid-cycle spotting around ovulation is considered a normal variant for some women. However, bleeding that is heavy, recurring, unpredictable, or associated with pain is not normal and should be evaluated by a healthcare provider.
Q: What does spotting between periods look like?
A: Spotting can appear as pink, brown, or light red discharge that doesn’t fill a pad. Brown spotting usually means older blood. Bright red spotting may indicate more active bleeding from the cervix or uterus.
Q: Can stress cause bleeding between periods?
A: Yes. Significant physical or emotional stress can disrupt the hypothalamic-pituitary-ovarian axis, interfering with normal ovulation and hormonal regulation. This can lead to irregular cycles and breakthrough bleeding.
Q: When should I be worried about spotting between periods?
A: You should seek prompt evaluation if bleeding is heavy, occurs after sex repeatedly, is accompanied by pelvic pain, happens after menopause, or occurs in three or more consecutive cycles. Postmenopausal bleeding requires urgent evaluation.
Q: Can STIs cause bleeding between periods?
A: Yes. Infections like chlamydia and gonorrhea can cause cervical inflammation that results in spotting or post-coital bleeding. Many STIs have no other symptoms, which is why testing is important.
Q: How is bleeding between periods diagnosed?
A: Diagnosis typically begins with a history, pregnancy test, and pelvic exam, followed by blood tests, transvaginal ultrasound, and if needed, endometrial biopsy or hysteroscopy.
Q: Can uterine fibroids cause bleeding between periods?
A: Yes, particularly submucosal fibroids that protrude into the uterine cavity. They can cause heavy periods, spotting between periods, and prolonged bleeding.
Q: Is bleeding between periods a sign of cancer?
A: In most cases, no. But cervical cancer, endometrial cancer, and — in rare cases — ovarian cancer can cause irregular bleeding. This is why any persistent or unexplained abnormal bleeding should be medically evaluated, especially in women over 40 or after menopause.
Q: Can birth control cause spotting between periods?
A: Yes. Breakthrough bleeding is common in the first 3 months of starting a new hormonal contraceptive. Progestin-only methods and missed pills are particularly associated with spotting.
Q: What is the medical term for bleeding between periods?
A: The correct terms are intermenstrual bleeding or metrorrhagia. The broader category of abnormal uterine bleeding is called AUB (abnormal uterine bleeding) or historically menometrorrhagia when it involves both irregular timing and excessive volume.