
If you’ve researched diaphragm birth control online, you’ve probably noticed something frustrating: every source seems to cite a different effectiveness number. One site says 88%. Another says 94%. A third says “70 to 99%.” None of that is necessarily wrong — but it leaves a lot of people unsure what to actually expect.
This guide lays out the diaphragm birth control pros and cons clearly, explains where those conflicting numbers come from, and covers the practical details — cost, prescriptions, and who shouldn’t use one — that get glossed over elsewhere. As always, this is general education, not a substitute for a conversation with your own healthcare provider, who can assess whether a diaphragm fits your specific health history.
What Is a Diaphragm and How Does It Work?
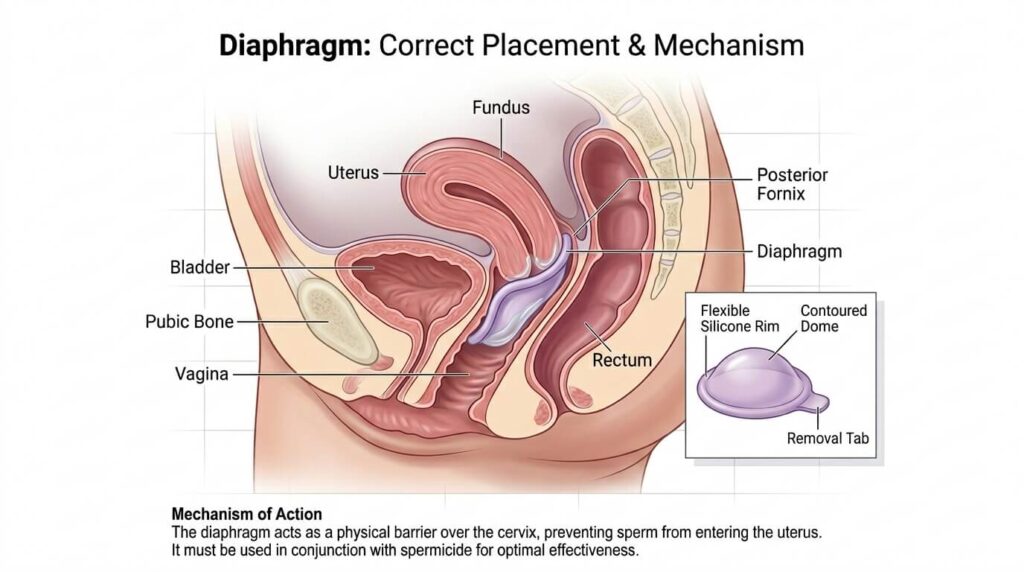
A diaphragm is a small, reusable, dome-shaped cup — typically made of silicone, since latex versions are largely no longer manufactured — that’s inserted into the vagina to cover the cervix. By physically blocking the opening to the uterus, it stops sperm from reaching an egg.
A diaphragm is never used alone. It’s always paired with spermicide, a cream or gel applied inside the dome and around the rim before insertion, which kills or immobilizes any sperm that gets past the barrier. Unlike hormonal methods, a diaphragm has no effect on your natural cycle and doesn’t require daily use — it’s inserted before sex and removed afterward.
Diaphragms require a prescription and a fitting from a healthcare provider, since an ill-fitting diaphragm is one of the most common reasons the method fails.
How Effective Is the Diaphragm, Really? (Clearing Up the Confusing Numbers)
Here’s why competitor sources disagree: they’re often citing different study populations, different diaphragm types, or conflating two distinct measures — perfect use and typical use.
Perfect Use vs. Typical Use
- Perfect use (used correctly, every single time, with spermicide reapplied as directed): around 94% effective, meaning roughly 6 out of 100 users become pregnant in a year.
- Typical use (which accounts for real-world inconsistency — forgetting spermicide, imperfect placement, not reapplying for repeat sex): effectiveness drops to roughly 82–88%, meaning somewhere between 12 and 18 out of 100 users become pregnant in a year.
That gap — wider than you’ll see for methods like the pill — exists because the diaphragm’s effectiveness depends heavily on correct placement and consistent spermicide use every time, not just remembering to take a daily pill. (Citation flag: cite the specific CDC or Planned Parenthood data table used for these figures in the published version, since exact percentages vary slightly by source and year.)

How It Compares to Other Birth Control Methods
| Method | Typical-Use Effectiveness | Hormonal? | STI Protection? |
|---|---|---|---|
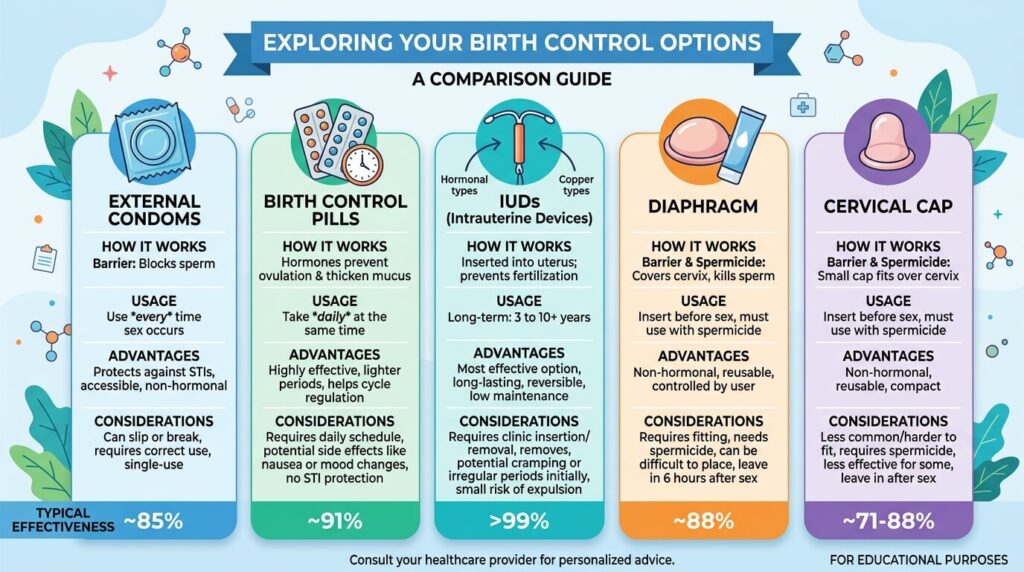
| Diaphragm + spermicide | ~82–88% | No | No |
| External condom | ~87% | No | Yes |
| Birth control pill | ~91–93% | Yes | No |
| Hormonal or copper IUD | >99% | Varies by type | No |
| Sterilization | >99% | No | No |
(Comparison takeaway: the diaphragm sits roughly in the same effectiveness range as condoms — better than nothing, meaningfully less effective than an IUD or sterilization, and entirely dependent on correct use every time.)
Diaphragm Birth Control: Pros
- Non-hormonal. A diaphragm doesn’t alter your natural hormone cycle, which makes it appealing if you can’t or don’t want to use hormonal methods.
- Safe while breastfeeding. Because it has no hormonal component, it doesn’t affect milk supply.
- Immediately reversible. There’s no waiting period to “get it out of your system” if you decide to try to conceive — you simply stop using it.
- Doesn’t require partner cooperation. It gives the person using it control over pregnancy prevention independent of whether a partner uses anything else.
- Reusable for up to two years with proper care, unlike single-use barrier methods like condoms or the sponge.
- Can be inserted ahead of time. It can go in up to several hours before sex, so it doesn’t have to interrupt the moment.
- Generally not felt by either partner when fitted and placed correctly.
Cons
- No STI protection. A diaphragm only addresses pregnancy prevention — pairing it with a condom is the only way to also reduce STI risk.
- Effectiveness drops significantly with imperfect use, and consistent, correct use is genuinely harder to maintain than with methods that don’t depend on per-use technique.
- Increased UTI risk for some users, particularly those already prone to urinary tract infections, since the rim can put pressure on the urethra.
- Small risk of toxic shock syndrome (TSS), a rare but serious bacterial illness — this is why diaphragms should never be left in longer than 24 hours.
- Requires a prescription and an in-person fitting, unlike over-the-counter options like condoms or spermicide alone.
- Spermicide must be reapplied for repeat intercourse, which some users find inconvenient or messy.
- Can shift out of place during particularly vigorous intercourse, reducing effectiveness for that act.
- Needs refitting after pregnancy, after a significant weight change, or roughly every one to two years.
How to Use a Diaphragm Correctly
- Wash your hands with mild, unscented soap before handling the diaphragm.
- Apply spermicide inside the dome and around the rim, following the amount specified on the product instructions.
- Fold the diaphragm in half and insert it into the vagina, guiding it back and up so it covers the cervix completely.
- Check placement with a finger — you should be able to feel your cervix through the dome, and the front rim should sit snugly behind the pubic bone.
- Leave it in place for at least 6 hours after sex, and never longer than 24 hours total.
- Reapply spermicide (without removing the diaphragm) if you have sex again before removing it.
- Remove, wash with mild soap and water, and air dry before storing it in its case.
Avoid oil-based lubricants (baby oil, certain lotions) with a diaphragm, since they can break down silicone and reduce effectiveness. (Author/expertise signal placeholder: this section should be reviewed and credited to a licensed OB/GYN or nurse practitioner, with their credentials noted, before publishing.)
Who Shouldn’t Use a Diaphragm?
A diaphragm may not be the right choice if you:
- Have given birth in the last six weeks, or had an abortion after the first trimester
- Have had recent cervical surgery
- Get frequent urinary tract infections
- Have a latex allergy and can’t access a latex-free option in your area
- Have anatomical changes to the vagina or cervix that affect fit (including some structural conditions present from birth)
- Aren’t confident you’ll use it correctly and consistently every time you have sex
If any of these apply to you, talk with your provider about alternative options — a diaphragm isn’t an all-or-nothing decision, and there are several non-hormonal and low-maintenance alternatives worth discussing.
Cost, Prescription, and Insurance: What to Expect
This is the piece almost no competitor page addresses directly. A few practical points:
- A prescription and fitting are required — you can’t buy a diaphragm over the counter in the way you can buy condoms or spermicide alone.
- Many insurance plans covering contraception treat the diaphragm as a covered method, though coverage for the fitting visit itself can vary by plan — it’s worth confirming with your insurer before the appointment. (Citation flag: insert a current source — e.g., HealthCare.gov’s contraceptive coverage page — confirming current ACA preventive-care coverage rules for diaphragms specifically.)
- Ongoing spermicide cost is the main recurring expense, since the diaphragm itself typically lasts one to two years before needing replacement.
- Refitting visits are needed periodically — after a pregnancy, a significant weight change, or per your provider’s recommended schedule — which is a recurring cost some other methods don’t carry.
Is a Diaphragm Right for You? A Quick Decision Checklist
A diaphragm is worth discussing with your provider if most of these apply to you:
- ✅ You want a non-hormonal method
- ✅ You’re breastfeeding and want a method that won’t affect milk supply
- ✅ You’re comfortable inserting and removing a vaginal device
- ✅ You can reliably plan ahead before sex (or insert it in advance)
- ✅ You don’t need STI protection from this method alone, or you’ll pair it with a condom
- ✅ You’re not currently dealing with frequent UTIs
If most of these don’t apply — for example, if you want a “set it and forget it” method, or you get UTIs often — a diaphragm is probably not your best first option, and it’s worth asking your provider about alternatives instead.
FAQ About Diaphragm Birth Control
How effective is a diaphragm at preventing pregnancy?
With perfect use, it’s about 94% effective. With typical use — accounting for real-world inconsistency — effectiveness drops to roughly 82–88%, meaning 12 to 18 out of 100 users may become pregnant in a year.
Do you need a prescription for a diaphragm?
Yes. Unlike condoms or spermicide alone, a diaphragm requires a prescription and an in-person fitting from a healthcare provider to ensure proper size and placement.
Can you feel a diaphragm during sex?
When fitted and inserted correctly, most users and their partners report not feeling it at all.
Does a diaphragm protect against STDs?
No. A diaphragm only prevents pregnancy. Pairing it with a condom is necessary for STI protection.
How long can you leave a diaphragm in?
It should stay in place for at least 6 hours after sex to allow the spermicide to work, but should never be left in for more than 24 hours total, due to the risk of toxic shock syndrome.
Can you use a diaphragm while breastfeeding?
Yes. Because it’s non-hormonal, a diaphragm doesn’t affect milk supply and is generally considered safe during breastfeeding — though it’s still worth confirming fit with your provider, since postpartum body changes can affect sizing.
What’s the difference between a diaphragm and a cervical cap?
Both are barrier devices used with spermicide to cover the cervix, but a cervical cap is smaller, fits more snugly directly over the cervix, and can typically be left in place longer than a diaphragm. A provider can help determine which shape fits better for your anatomy.
Is the diaphragm a good birth control option in 2026?
It remains a legitimate option for people who specifically want a non-hormonal, on-demand, reversible method, even though it’s used less often today than methods like IUDs or the pill, largely because those alternatives don’t require per-use technique.

Conclusion: Talk to Your Provider About What Fits Your Life
The diaphragm isn’t the most effective birth control method available, and it isn’t the lowest-maintenance one — but for the right person, it offers something hormonal methods and IUDs don’t: a non-hormonal, fully reversible, on-demand option that puts the user in direct control. The honest answer to “is it right for me” depends less on a single effectiveness percentage and more on how consistently you can use it and what trade-offs matter most to you.
If you’re considering a diaphragm, the next right step is a conversation with your OB/GYN or healthcare provider about a proper fitting and whether your health history affects your options.