
If you’ve been diagnosed with uterine prolapse and you’re dreaming of a baby, the first question is usually the scariest one: is this even possible? The short answer is yes — most women with uterine prolapse can get pregnant, carry a pregnancy, and deliver a healthy baby. But the full answer is more nuanced, and it depends on how severe your prolapse is, how it’s managed, and the kind of care you get along the way.
This guide walks through everything you need to know: how prolapse affects fertility, what happens to a prolapsed uterus during pregnancy, the real risks involved, how doctors manage the condition trimester by trimester, delivery options, and what recovery looks like afterward. It draws on current medical literature, case studies, and clinical guidance so you have one complete, trustworthy resource instead of piecing together fragments from a dozen different sites.
Quick Answer
Yes, you can get pregnant with uterine prolapse, including most cases of mild to moderate prolapse. Severe (stage 3–4) prolapse can make conception physically harder and raises the risk of complications during pregnancy, but successful pregnancies have been documented even in advanced cases. Medical supervision, a pessary if needed, and a personalized birth plan are the keys to a safe outcome.
What Is Uterine Prolapse, Exactly?
Uterine prolapse happens when the muscles and ligaments that hold the uterus in place — primarily the uterosacral and cardinal ligaments and the pelvic floor muscles — weaken or stretch. Without that support, the uterus slips down the vaginal canal. In mild cases it barely shifts; in severe cases, it protrudes outside the vaginal opening entirely.
Uterine prolapse is one type of a broader condition called pelvic organ prolapse (POP), which can also involve the bladder (cystocele), rectum (rectocele), or the top of the vagina after a hysterectomy (vaginal vault prolapse). These conditions often overlap, since the same supportive tissues hold multiple pelvic organs in place.

How Common Is It?
Pelvic organ prolapse is common in the general population, especially after childbirth or with age, but uterine prolapse that develops during an active pregnancy is rare. Clinical literature estimates it occurs in roughly 1 in 10,000 to 15,000 pregnancies. Far more common is the scenario this article focuses on: a woman who already has uterine prolapse before she conceives.
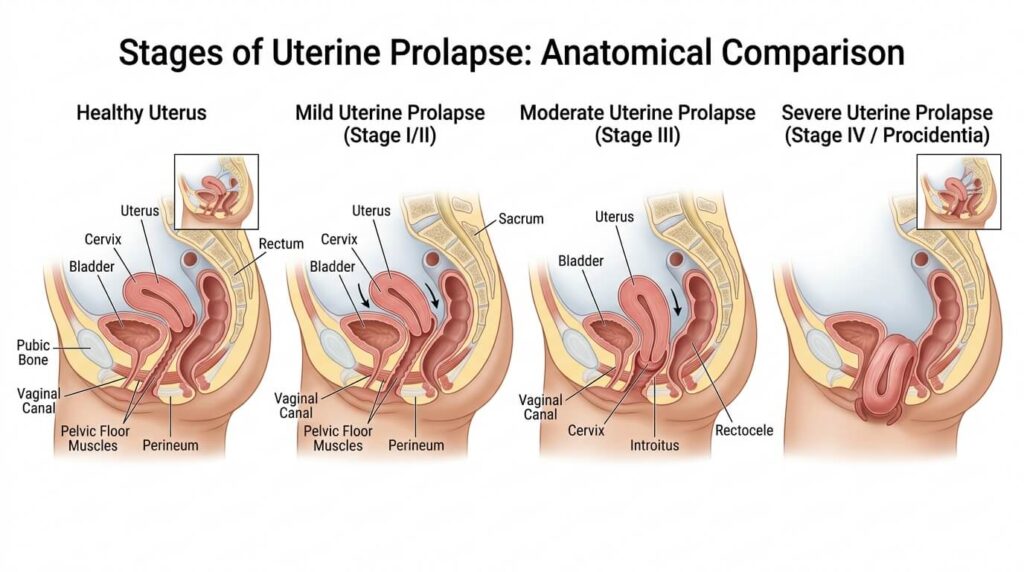
Stages of Uterine Prolapse (POP-Q System)
Doctors classify prolapse severity using the Pelvic Organ Prolapse Quantification (POP-Q) system, which measures how far the uterus has descended relative to the hymen.
| Stage | Description | Typical Symptoms |
|---|---|---|
| Stage 0 | No prolapse; normal support | None |
| Stage 1 | Mild — uterus sits more than 1 cm above the hymen | Often none, sometimes mild heaviness |
| Stage 2 | Moderate — uterus is within 1 cm of the hymen | Vaginal bulge sensation, pressure |
| Stage 3 | Severe — uterus extends more than 1 cm beyond the hymen | Visible bulge, discomfort, urinary issues |
| Stage 4 | Complete prolapse — uterus protrudes fully outside the vagina | Tissue exposure, irritation, difficulty with hygiene and intercourse |
Most prolapse becomes noticeably symptomatic once it reaches stage 2 or beyond, which is also the point where it can start to interfere with comfortable intercourse and conception.
Does Uterine Prolapse Affect Fertility?
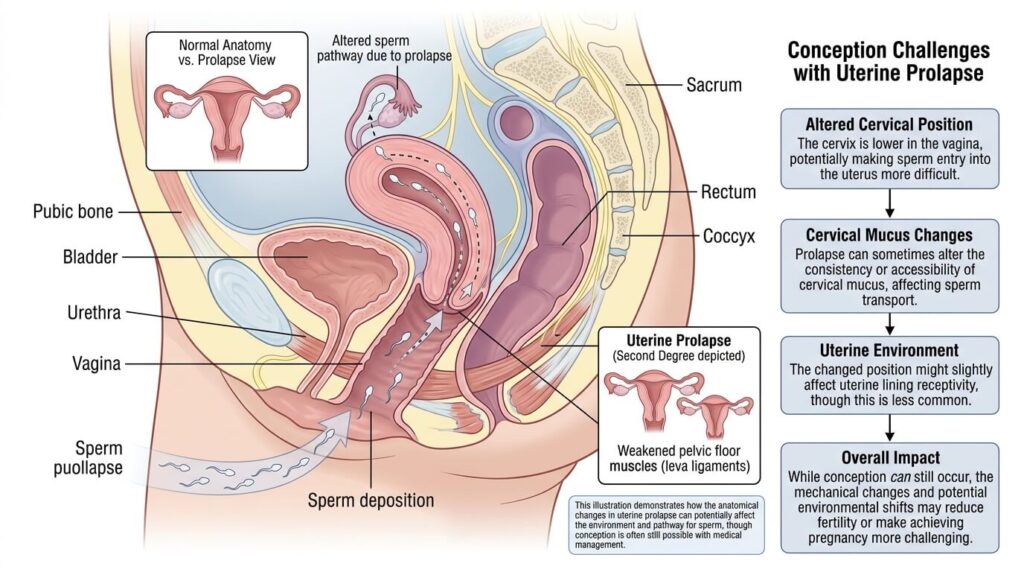
Uterine prolapse does not directly damage the ovaries, fallopian tubes, or uterine lining, so it doesn’t cause infertility in the way a blocked tube or hormonal disorder would. But it can create mechanical barriers to conception, particularly in moderate-to-severe cases.
Why Conception Can Be Harder
- Sperm exposure to air. When the uterus and cervix sit low in or outside the vagina, semen deposited during intercourse can be pushed toward — or out of — the vaginal opening instead of staying near the cervix. Sperm need a warm, moist environment to survive; exposure to air shortens their lifespan dramatically.
- Painful or difficult intercourse. A bulging uterus or vaginal walls can make penetration uncomfortable, which may reduce the frequency or completion of intercourse during the fertile window.
- Cervical positioning. In advanced prolapse, the cervix may be displaced far from its normal position, making it harder for sperm to find their way through the cervical canal.
When Fertility Treatment Helps
For women trying to conceive with moderate-to-severe prolapse, some clinicians recommend treating the prolapse first — through pelvic floor therapy, a pessary, or in select cases, a uterus-preserving surgery called hysteropexy — before actively trying. Hysteropexy resuspends the uterus without removing it, which matters for anyone who still wants to carry a pregnancy. Several published series describe women becoming pregnant and delivering successfully after this procedure.
If you’re not conceiving despite regular intercourse, prolapse may be a contributing factor, but it’s worth ruling out other causes (ovulation issues, tubal factors, male-factor infertility) with a fertility specialist rather than assuming prolapse is the sole reason.
Can a Prolapsed Uterus Hold a Pregnancy?
Yes. The uterus is a muscular organ, and pregnancy itself often changes the physics of prolapse in a woman’s favor. As the uterus grows in early pregnancy, it frequently becomes too large to continue descending through the vaginal canal, and in many documented cases the prolapse temporarily improves or fully resolves by the second trimester, since the growing uterus is “trapped” above the pelvic floor by its own size.
This doesn’t apply to every case — some women experience worsening prolapse, especially in the first trimester before the uterus enlarges enough to self-correct, or after delivery once it shrinks back down. But it explains why many pregnancies in women with pre-existing prolapse proceed without major incident.

Risks and Complications to Know About
Being informed about risks isn’t meant to frighten you — it’s meant to help you and your medical team watch for the right things at the right times.
First-Trimester Risks
- Incarcerated uterus. Rarely, the enlarging uterus gets trapped below the pelvic brim before it has room to rise into the abdomen, which can cause severe pain, urinary retention, or miscarriage if untreated.
- Increased miscarriage risk in cases of severe, unmanaged prolapse, largely tied to mechanical strain and associated infection risk rather than the prolapse itself.
Throughout Pregnancy
- Cervical changes. Pregnancy hormones soften and lengthen the cervix, which can make an existing prolapse feel more pronounced even while the uterus itself rises.
- Urinary symptoms. Pressure on the bladder can worsen urinary frequency, urgency, or incontinence beyond what’s typical in pregnancy.
- Vaginal tissue exposure and infection. If the cervix or uterine tissue stays outside the vaginal opening for extended periods, it can dry out, ulcerate, or become infected — a condition sometimes called decubitus ulceration. Keeping the area clean and using a pessary, if recommended, reduces this risk.
- Preterm labor. Chronic irritation or infection from exposed tissue has been linked, in some case reports, to a higher chance of preterm contractions.
Labor and Delivery Risks
- Cervical dystocia. In rare cases, a severely prolapsed or edematous cervix fails to dilate normally, prolonging labor.
- Cervical laceration or uterine rupture. Extremely rare, but case literature notes these as possible complications in advanced, unmanaged prolapse during vaginal delivery.
- Obstructed labor, if the prolapse prevents normal descent of the baby through the birth canal.
It’s worth emphasizing: these are documented possibilities, not the expected outcome. The majority of women with mild-to-moderate prolapse have unremarkable pregnancies and vaginal deliveries.
How Doctors Manage Pregnancy With Uterine Prolapse
Before You Conceive
- A full pelvic exam and POP-Q staging to establish a baseline.
- Pelvic floor physical therapy, which can strengthen support and sometimes improve mild prolapse before pregnancy even starts.
- Discussion of whether a pessary or, in select cases, hysteropexy makes sense before trying to conceive.
During Pregnancy
- Regular monitoring. More frequent prenatal visits than a standard low-risk pregnancy are common, particularly through the first and third trimesters.
- Pelvic rest recommendations. Many providers advise avoiding heavy lifting, prolonged standing, high-impact exercise, and sometimes intercourse if the prolapse is significant.
- Pessary use. A vaginal pessary — a removable silicone or plastic device — can be fitted to hold the uterus in a more normal position, ease discomfort, and reduce the risk of tissue exposure. It’s a non-surgical option that’s safe to use through most of pregnancy and is generally removed before labor.
- Pelvic floor exercises (Kegels). Strengthening the levator ani and surrounding muscles can ease symptoms and may help limit how much the prolapse worsens.
- Nutrition and bowel management. A diet rich in fiber and adequate water intake helps prevent constipation and straining, which adds pressure to an already weakened pelvic floor.
- Hygiene care. If any tissue protrudes outside the vagina, gentle cleaning and provider-recommended barrier creams reduce irritation and infection risk.
Labor and Delivery Planning
There is no single “correct” delivery method for every woman with uterine prolapse — it depends on the stage of prolapse, how it’s behaving near term, and obstetric factors unrelated to the prolapse itself.
- Vaginal delivery is often possible and is not automatically ruled out by a prolapse diagnosis, even when the prolapse is fairly advanced, provided there’s no obstruction and the cervix dilates normally.
- Cesarean delivery may be recommended electively near term in cases of severe, persistent prolapse, particularly if the uterus has remained outside the vaginal canal late in pregnancy, since this can reduce the risk of cervical laceration, obstructed labor, or uterine rupture. Some published case series specifically favor a planned cesarean for fourth-degree (complete) prolapse.
Your obstetrician — ideally one with urogynecology experience or in consultation with a urogynecologist — should walk you through which option fits your specific anatomy and history.
Postpartum: What Happens to the Prolapse After Birth?
Pregnancy and delivery affect prolapse in different ways depending on the individual:
- Some women see improvement. In documented cases, prolapse that was present before pregnancy did not recur, or recurred much less severely, after delivery — particularly after a cesarean section.
- Some women see no change, with the prolapse returning to its pre-pregnancy baseline once the uterus shrinks back (involutes) over the following weeks.
- Some women see worsening, especially after a vaginal delivery, since the pelvic floor absorbs significant strain during labor.
A pessary is often reinserted in the days after delivery to support the uterus through the involution period, and pelvic floor physical therapy is commonly recommended starting around six weeks postpartum, once cleared by a provider.
Can You Prevent Uterine Prolapse Before or During Pregnancy?
While you can’t always prevent prolapse — genetics, connective tissue strength, and prior deliveries all play a role — these habits meaningfully lower the risk or slow progression:
- Pelvic floor (Kegel) exercises, done consistently before, during, and after pregnancy.
- Maintaining a healthy weight, since excess weight adds chronic pressure on the pelvic floor.
- Treating chronic cough or constipation promptly, since repeated straining is one of the biggest contributors to prolapse.
- Avoiding heavy lifting or learning safer lifting mechanics that engage the legs rather than the abdomen.
- Spacing pregnancies and allowing adequate pelvic floor recovery time between vaginal deliveries.
- Attending postpartum pelvic floor checks, even if you feel fine, since early-stage prolapse is often symptom-free.
Uterine Prolapse vs. Other Pelvic Floor Conditions: How They Compare
| Condition | What Prolapses | Effect on Fertility | Effect on Pregnancy |
|---|---|---|---|
| Uterine prolapse | Uterus and cervix descend into/through the vagina | Possible mechanical barrier in moderate–severe cases | Often improves in 2nd trimester; delivery method depends on severity |
| Cystocele (bladder prolapse) | Bladder bulges into the front vaginal wall | Minimal direct effect | Can worsen urinary symptoms during pregnancy |
| Rectocele | Rectum bulges into the back vaginal wall | Minimal direct effect | Can worsen constipation and straining risk |
| Vaginal vault prolapse | Top of vagina (post-hysterectomy) descends | Not applicable (uterus already removed) | Not applicable |
| Cervical elongation (without full prolapse) | Cervix lengthens without major descent | Usually minimal | May be mistaken for worsening prolapse late in pregnancy |
Common Mistakes Women Make With Prolapse and Pregnancy Planning
- Assuming prolapse equals infertility and giving up on natural conception without ever getting a tailored evaluation.
- Skipping pre-pregnancy pelvic floor therapy, which is often more effective when started before conception than after symptoms intensify.
- Ignoring a pessary fitting out of discomfort with the idea, when a well-fitted pessary can meaningfully reduce pregnancy complications.
- Ramping up high-impact exercise during pregnancy without discussing it with a provider familiar with the prolapse.
- Waiting too long to mention symptoms like increased bulging, bleeding, or discharge to a provider, assuming it’s “just pregnancy.”
- Assuming a cesarean is automatically required. Many women with prolapse deliver vaginally without issue; the decision should be individualized, not automatic.
Expert Tips for a Safer Pregnancy With Uterine Prolapse
- Get staged with a formal POP-Q exam early, ideally before conceiving, so you and your provider have a clear baseline to track changes against.
- Ask specifically whether a pessary is appropriate for your stage of prolapse — it’s one of the most effective non-surgical tools available throughout pregnancy.
- Build a relationship with a urogynecologist alongside your obstetrician if your prolapse is stage 2 or higher.
- Keep a symptom diary noting bulge size, discomfort level, and any bleeding or discharge to share at prenatal visits.
- Discuss your birth plan by the third trimester rather than waiting until labor begins, since delivery method decisions often need to be made in advance for advanced prolapse.
Frequently Asked Questions
Can you get pregnant with a uterine prolapse?
Yes. Most women with mild to moderate uterine prolapse conceive without medical intervention. Severe prolapse can make conception physically harder, but pregnancy is still possible, sometimes with help from a pessary or corrective surgery beforehand.
Does uterine prolapse cause infertility?
Not directly. It doesn’t affect egg quality, ovulation, or sperm production. It can create mechanical obstacles to conception in advanced cases, which is different from true infertility.
Will pregnancy make my prolapse worse?
It can go either way. Many women see their prolapse improve in the second trimester as the growing uterus rises out of the pelvis, while others notice it worsens, particularly late in the third trimester or after a vaginal delivery.
Is it safe to have a vaginal delivery with uterine prolapse?
Often, yes. Vaginal delivery is not automatically ruled out by prolapse, even advanced prolapse. Your provider will weigh your specific anatomy, how the prolapse is behaving near term, and any obstetric risk factors.
Do I need a cesarean section if I have uterine prolapse?
Not necessarily. A cesarean may be recommended for severe, persistent prolapse or specific complications like cervical laceration risk, but many women with prolapse deliver vaginally.
Can a pessary be worn safely during pregnancy?
Yes, pessaries are commonly used throughout pregnancy to support the uterus and reduce symptoms. They are typically removed before labor and may be refitted after delivery.
What does it feel like to be pregnant with uterine prolapse?
Many women describe a sensation of vaginal pressure, heaviness, or a visible bulge that may fluctuate with activity, time of day, and trimester. Symptoms often ease mid-pregnancy and can return late in the third trimester.
Can uterine prolapse cause a miscarriage?
It’s an uncommon but documented risk, mainly tied to severe, unmanaged cases involving an incarcerated uterus or significant infection. Most pregnancies with mild-to-moderate prolapse are not at meaningfully elevated miscarriage risk.
Does hysteropexy affect future pregnancies?
Hysteropexy is specifically designed to preserve the uterus while correcting prolapse, and successful pregnancies after the procedure have been documented in medical literature. It’s generally considered for women who want to retain fertility, unlike a hysterectomy.
How common is uterine prolapse during pregnancy?
Prolapse that develops for the first time during pregnancy is rare, estimated at about 1 in 10,000–15,000 pregnancies. Pre-existing prolapse that a woman carries into pregnancy is more common, though exact prevalence varies by population.
Can exercise help with prolapse while trying to conceive?
Yes. Pelvic floor (Kegel) exercises and guided pelvic floor physical therapy are commonly recommended both before conception and throughout pregnancy to support pelvic muscles and ease symptoms.
What’s the difference between uterine prolapse and pelvic organ prolapse?
Uterine prolapse is one specific type of pelvic organ prolapse, referring specifically to the uterus and cervix descending. Pelvic organ prolapse is the broader term covering the bladder, rectum, and uterus or vaginal vault.
Will my prolapse go away after I give birth?
Sometimes. Some women see prolapse improve or fully resolve after delivery, especially after a cesarean section, while others see it return to baseline or worsen, particularly after vaginal birth. Postpartum pelvic floor therapy can help either way.
Is sex painful with uterine prolapse, and does that affect conception?
For some women, yes, particularly with moderate-to-severe prolapse, and this can indirectly make conception more difficult if it limits frequency or comfort of intercourse. A pessary, lubrication, and position adjustments can often help.
Should I see a specialist before trying to conceive with prolapse?
It’s a reasonable step, especially for stage 2 prolapse or higher. A urogynecologist can stage your prolapse, discuss pessary fitting or hysteropexy, and help you plan conception with fewer surprises.
