Confused about the stages of labor? Get clear timelines, dilation charts, pain-relief options, and warning signs for every phase of childbirth. Nobody hands you a script when labor starts. One moment you’re timing a backache that might be nothing, and a few hours (or days) later you’re being told to push. Understanding the stages of labor — what’s happening to your body, how long each part tends to last, and what your care team is actually watching for — turns that uncertainty into something you can navigate with confidence.
Labor is generally divided into three stages: dilation of the cervix, the birth of the baby, and delivery of the placenta. Many clinicians also recognize an important fourth stage — the first hours after birth — that’s just as critical for your safety even though it rarely gets discussed. This guide walks through every stage and phase in detail, explains the science behind why labor happens the way it does, and answers the questions women ask most often before, during, and after delivery.
Quick Answer: What Are the Stages of Labor?
Labor unfolds in three core stages, sometimes extended to four:
- Stage 1 — Dilation and effacement: From the start of regular contractions until the cervix is fully open (10 cm). This stage has three phases: early labor, active labor, and transition.
- Stage 2 — Pushing and birth: From full dilation until your baby is born.
- Stage 3 — Delivery of the placenta: From the birth of your baby until the placenta is delivered.
- Stage 4 — Immediate recovery: The first one to three hours after the placenta is delivered, when your body begins to stabilize and bonding begins.
No two labors are identical, and the timeline below reflects averages, not guarantees.
How Do You Know Labor Is Starting? Pre-Labor Signs
Before contractions become regular, your body often gives a few advance signals that birth is approaching, usually within days to a couple of weeks:
- Lightening (dropping): The baby settles lower into the pelvis, which can make breathing easier but increase pelvic pressure.
- Nesting instinct: A sudden urge to clean, organize, or prepare the home. Not everyone experiences this.
- Cervical changes: Your provider may note softening, thinning, or slight opening of the cervix during an exam.
- Bloody show: A small amount of pink or blood-tinged mucus discharge as the mucus plug loosens from the cervical opening.
- Backaches and loose stools: Hormonal shifts can cause lower back discomfort and diarrhea-like bowel changes.
These signs don’t guarantee labor is imminent — some people experience them for days before anything else happens, and others go straight into contractions without noticing any of them.
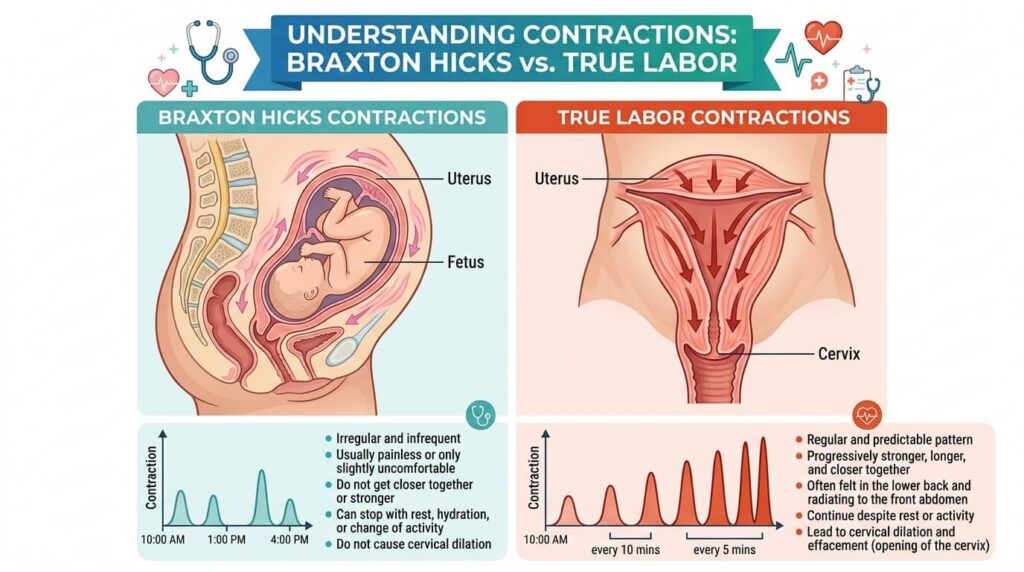
True Labor vs. False Labor (Braxton Hicks)
One of the most common sources of confusion in late pregnancy is distinguishing true labor from Braxton Hicks contractions, often called “practice contractions.” The clearest way to tell them apart is to track three things: frequency, duration, and intensity.
| Feature | Braxton Hicks (False Labor) | True Labor |
|---|---|---|
| Pattern | Irregular, unpredictable | Regular, gets more frequent |
| Intensity | Stays the same or fades | Steadily increases |
| Effect of movement | Often eases with walking, rest, or position change | Continues or worsens regardless of activity |
| Cervical change | None | Progressive dilation and effacement |
| Location | Usually front of abdomen | Often starts in the back, wraps to the front |
If contractions are getting closer together, lasting longer, and intensifying no matter what position you try, that’s a strong indicator labor has truly begun.
What Triggers Labor?
The exact mechanism that starts labor isn’t fully understood, but research points to a cascade of biochemical signals between the fetus, the placenta, and the uterus. Two hormone-like substances play the leading roles:
- Prostaglandins: Produced by uterine cells, these help soften and dilate the cervix while triggering uterine contractions.
- Oxytocin: Released by the pituitary gland (and given synthetically as Pitocin during induction), oxytocin stimulates and strengthens contractions.
For most pregnancies, this process begins naturally somewhere between 37 and 42 weeks. When it doesn’t start on its own and there’s a medical reason to move things along, a provider may recommend labor induction using synthetic oxytocin, cervical ripening agents, or membrane rupture.

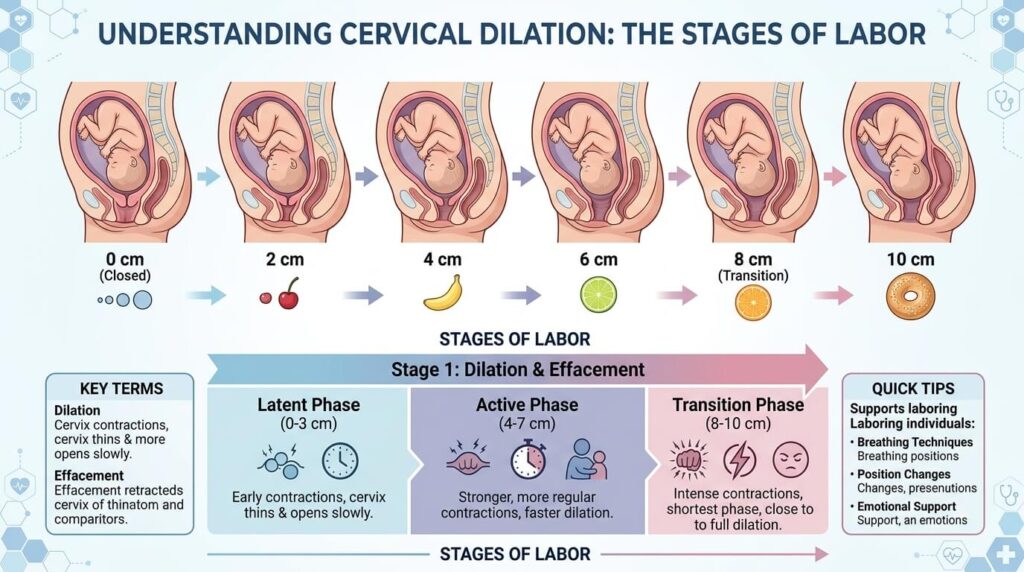
Stage 1 of Labor: Dilation and Effacement
The first stage is the longest part of labor for almost everyone. It begins with the onset of regular contractions and ends only when the cervix has fully dilated to 10 centimeters and completely effaced (thinned). Total length commonly ranges from 12 to 19 hours, though it’s often considerably shorter for people who have given birth before.
This stage breaks down into three recognizable phases.
Early (Latent) Labor
During early labor, contractions begin softening and opening the cervix, generally up to about 6 centimeters under current obstetric guidelines (older references sometimes cite a 3 to 4 cm cutoff, but most modern care teams now use 6 cm as the start of active labor). Contractions in this phase tend to be mild to moderate, spaced five to twenty minutes apart, and may not yet follow a consistent pattern.
How long it lasts: Highly variable — anywhere from several hours to a couple of days, and it can stop and restart. It’s typically faster for second or later births.
What helps: Most people manage early labor comfortably at home. Useful strategies include:
- Walking or gentle movement
- A warm shower or bath
- Eating a light meal if your provider hasn’t restricted food
- Resting or even sleeping if contractions allow it
- Practicing breathing techniques learned in childbirth classes
- Changing positions frequently
There’s usually no need to head to the hospital yet unless your water breaks, you notice heavy bleeding, or your provider has given you specific instructions to come in sooner.
Active Labor
Active labor is when things noticeably intensify. The cervix dilates from roughly 6 cm to 10 cm, contractions become stronger, longer, and closer together — often three to five minutes apart, lasting 45 to 90 seconds — and progress becomes more predictable, averaging about 1 centimeter of dilation per hour.
How long it lasts: Typically 4 to 8 hours, though first-time labors can run longer.
What helps: This is generally the point at which your care provider will want you at the hospital or birthing center. Comfort measures shift toward:
- Birthing balls or peanut balls for hip mobility
- Continuous or intermittent support from a partner, nurse, or doula
- Massage between contractions
- Position changes (hands and knees, side-lying, leaning forward)
- Pain relief options, whether non-medicated or medicated (covered in detail below)
If you’re planning a C-section or considering an epidural, your team may limit you to clear liquids — water, ice chips, or popsicles — rather than solid food during this phase.
Transition
Transition is the final, most intense part of the first stage, generally covering 8 to 10 cm of dilation. Contractions during transition can last 60 to 90 seconds with as little as 30 seconds to 2 minutes of rest in between. It’s common to experience nausea, trembling, chills, intense pressure in the lower back and rectum, and a strong urge to push.
How long it lasts: Usually the shortest phase — often 15 minutes to 2 hours.
What helps: Short, focused breathing (panting or blowing) can help you avoid pushing before your cervix is fully open, which matters because pushing too early can cause cervical swelling and slow delivery. Tell your nurse or provider the moment you feel pressure to push so they can confirm you’re fully dilated.
Stage 1 Phase Comparison Table
| Phase | Cervical Dilation | Contraction Frequency | Contraction Length | Typical Duration |
|---|---|---|---|---|
| Early labor | 0–6 cm | Every 5–20 minutes | 30–45 seconds | Hours to 1–2 days |
| Active labor | 6–10 cm | Every 3–5 minutes | 45–90 seconds | 4–8 hours |
| Transition | 8–10 cm | Every 30 sec–2 min | 60–90 seconds | 15 minutes–2 hours |
Stage 2 of Labor: Pushing and Birth
The second stage starts the moment your cervix is fully dilated and ends with the birth of your baby. It can be as short as a few minutes or extend over a few hours, and tends to take longer for first-time parents and for those who have an epidural.
What typically happens during this stage:
- Contractions occur every two to five minutes, lasting 60 to 90 seconds, with a rest period in between when you can recover.
- You’ll be coached to push during contractions — either when your provider tells you to bear down, or based on your own urge, depending on your care team’s approach.
- The baby descends through the birth canal. At some point, your provider may ask you to ease off pushing so vaginal tissue can stretch gradually rather than tear.
- Crowning occurs when the baby’s head becomes visible at the vaginal opening.
- After the head is delivered, the shoulders and body follow, usually within moments.
- The umbilical cord is clamped and cut — often with a short delay of 30 to 180 seconds, since delayed cord clamping allows extra blood to transfer from the placenta, boosting the baby’s iron stores and lowering the risk of anemia.
Pushing Positions
There’s no single “correct” position for pushing, and trying a few can help you find what works:
- Squatting: Uses gravity and can widen the pelvic outlet.
- Side-lying: Useful if you have an epidural or need to slow a fast second stage.
- Hands and knees: Can relieve back pressure, especially helpful for posterior (back labor) positioning.
- Semi-sitting or supported sitting: A common default in hospital beds, allowing visual feedback and easy monitoring.
- Kneeling, leaning on a partner, or using a birthing bar: Combines upright benefits with extra support.
Stage 3 of Labor: Delivery of the Placenta
The third stage begins right after your baby is born and ends when the placenta is delivered. It’s the shortest stage of labor, usually completed within 5 to 30 minutes.
Mild contractions resume a few minutes after birth to help separate the placenta from the uterine wall. You may be asked to push gently one more time, or your provider may apply gentle pressure to your abdomen to help it along. Many hospitals practice “active management” of this stage — giving a dose of oxytocin and applying controlled cord traction — because it reduces the risk of excessive bleeding compared with waiting for the placenta to deliver entirely on its own.
After delivery, your provider examines the placenta to confirm it’s intact. Any retained fragments must be removed, since leftover tissue raises the risk of infection and hemorrhage. If you tore or had an episiotomy, repair happens at this point, typically under local anesthetic if you didn’t already have an epidural.
When this stage is considered abnormal: Most providers intervene if the placenta hasn’t delivered within 30 minutes, since a retained placenta increases the risk of significant blood loss.
Stage 4: The Hour(s) Right After Birth
Many people are never told about a fourth stage of labor, but it’s a meaningful part of recovery that clinicians actively monitor. It covers roughly the first one to three hours after the placenta is delivered.
During this window:
- Your uterus continues contracting and a nurse may periodically massage your abdomen to help it firm up and limit bleeding.
- Vital signs — blood pressure, pulse, and bleeding — are checked frequently.
- This is often the first opportunity for skin-to-skin contact and, if you’re planning to, your first attempt at breastfeeding.
- Shaking, chills, or exhaustion are common and generally resolve within an hour or two.
Bonding can happen here, but don’t worry if you feel disoriented or simply relieved rather than overwhelmed with emotion right away — there’s no “correct” reaction in the fourth stage.

How Long Does Labor Actually Last?
There’s no universal timeline, but typical ranges are:
- First-time births: Often 12 to 24 hours total, sometimes longer.
- Subsequent births: Often shorter, averaging 8 to 10 hours.
- Precipitous (rapid) labor: A small number of people skip much of early labor and move through active labor, birth, and placenta delivery in roughly 3 to 5 hours total.
Several factors influence how long labor takes: whether it’s a first birth, the baby’s position and size, the strength and regularity of contractions, whether labor was induced, pain medication, and your pelvic anatomy.
When Labor Doesn’t Follow the Typical Pattern: Prolonged and Abnormal Labor
Care providers use specific clinical benchmarks to decide when labor has stalled enough to warrant intervention. These thresholds differ slightly by stage and by whether it’s a first birth:
Stage 1 (early/latent phase) is considered prolonged if:
- It lasts more than 20 hours for a first birth, or
- More than 14 hours for someone who has given birth before.
Active labor is considered to have stalled (arrest of dilation) if:
- The cervix doesn’t progress past 6 cm after 4 hours of strong, regular contractions with ruptured membranes, or
- After 6 hours of contractions with ruptured membranes despite receiving oxytocin augmentation.
Stage 2 is considered prolonged if:
- It exceeds 3 hours without an epidural (4 hours with one) for a first birth, or
- 2 hours without an epidural (3 hours with one) for someone who has given birth before.
Stage 3 is considered abnormal if the placenta hasn’t delivered within 30 minutes of the baby’s birth.
When labor stalls, providers may recommend walking or position changes, breaking the water if it hasn’t happened naturally, augmenting contractions with oxytocin, or — if the baby shows signs of distress or labor truly fails to progress — a C-section.
Special Labor Scenarios
Induced Labor
If labor doesn’t start on its own by a certain point, or if there’s a medical reason to deliver sooner, your provider may induce labor using methods such as cervical ripening medication, a Foley balloon, membrane sweeping, artificially rupturing the membranes, or an IV oxytocin drip. Induced labors can still progress through the same three stages, though the early phase is often compressed or skipped.
Cesarean Birth (C-Section)
Not every labor ends in vaginal delivery. You might go through stage 1 contractions and then need an unplanned C-section if labor stalls or the baby shows signs of distress, or you may have a planned C-section and never experience early labor or pushing at all. In a C-section, the surgical team delivers the placenta directly during the procedure rather than waiting for a natural third stage.
VBAC (Vaginal Birth After Cesarean)
Many people who’ve had a prior C-section can safely labor and deliver vaginally in a later pregnancy. A VBAC generally follows the same staged process described above, though hospitals typically monitor contractions and the uterine scar more closely.
Multiples
With twins or higher-order multiples, the first and second stages may unfold differently — contractions can feel different earlier, and there’s often a short pause between delivering the first and second baby during stage 2.
Pain Management Options During Labor
Pain tolerance and preference vary enormously, and there’s no “right” amount of pain relief to use. Most options fall into two categories.
Non-Medicated (Natural) Methods
- Breathing and relaxation techniques
- Warm water — a shower, bath, or birthing tub
- Massage and counter-pressure
- Heat or cold packs
- Continuous support from a partner or doula
- Frequent position changes
- Visualization and guided imagery
- Aromatherapy
- Music
Medicated Methods
| Method | How It Works | Typical Use |
|---|---|---|
| Opioids (e.g., morphine, fentanyl) | Injected into a vein or muscle to dull pain | Early to active labor |
| Nitrous oxide (“laughing gas”) | Inhaled gas that reduces pain perception without full numbness | Any point; effects wear off quickly when stopped |
| Epidural | Catheter delivers anesthetic/narcotic into the lower back, numbing from the waist down | Active labor onward |
| Spinal block | Single injection into spinal fluid for rapid numbing | Often used for C-sections |
| Pudendal block | Local anesthetic injected near the pudendal nerve | Late stage 2, just before delivery |
| General anesthesia | Full loss of consciousness via medication and muscle relaxants | Rare; emergency C-sections only |
Talk with your care team ahead of time about what’s available at your hospital or birthing center, since not every option is offered everywhere, and preferences can always change once you’re actually in labor.
When to Go to the Hospital or Birthing Center
Your provider will likely give personalized guidance, but general signs that it’s time include:
- Contractions are coming about every five minutes, lasting roughly a minute, for at least an hour (often summarized as the “5-1-1 rule”)
- Your water breaks, regardless of whether contractions have started
- You notice bright red or heavy vaginal bleeding
- Lower back pain or cramping intensifies and won’t ease up
- You notice a significant decrease in fetal movement
Seek emergency care immediately if you experience chest pain, severe dizziness or fainting, shortness of breath, sudden swelling of the face, hands, or legs, or severe nausea and vomiting alongside other labor symptoms — these can signal complications like preeclampsia that need urgent evaluation.

What Happens When You Arrive at the Hospital
Knowing the admission routine in advance can make it feel less overwhelming:
- You check in at the labor and delivery desk and are usually taken to a triage room first.
- A nurse checks your pulse, blood pressure, and temperature.
- An external fetal monitor is placed on your abdomen to track contractions and your baby’s heart rate.
- A cervical exam determines how far labor has progressed.
- An IV line may be placed in case you need fluids or medication.
- Once admitted, you’re moved to a labor, delivery, and recovery (LDR) room, where you’ll stay through delivery and the early postpartum period.
Common Mistakes to Avoid During Labor
- Arriving at the hospital too early. Going in during mild, irregular early labor can mean being sent home, which can feel discouraging. Timing contractions carefully helps you judge the right moment.
- Skipping food and hydration in early labor. Unless your provider has restricted intake, eating light and staying hydrated during early labor helps maintain energy for active labor.
- Holding your breath while pushing. Long breath-holds can reduce oxygen flow; many providers now encourage more natural, shorter pushing breaths guided by your own urge.
- Staying in one position too long. Movement and position changes can speed progress and ease pain, particularly during active labor.
- Not communicating pain levels honestly. Pain management works best when your team knows exactly what you’re feeling and when.
- Assuming all labors follow the textbook timeline. Comparing your labor to a friend’s or to a chart can create unnecessary anxiety — every labor is different.
The Role of Your Support Team
A consistent support person — a partner, family member, friend, or trained doula — can measurably improve comfort and confidence throughout labor. Doulas specifically offer continuous physical and emotional support (though not medical care), while midwives and OB-GYNs manage the clinical side of labor and delivery. Discussing roles and expectations with your support team before labor begins helps everyone work together smoothly when the time comes.
Glossary of Key Labor Terms
- Dilation: How open the cervix is, measured in centimeters from 0 to 10.
- Effacement: How thin the cervix has become, measured in percentages from 0% to 100%.
- Station: How far the baby’s head has descended into the pelvis, measured relative to the ischial spines.
- Crowning: The moment the baby’s head becomes visible at the vaginal opening.
- Bloody show: Pink or blood-tinged mucus discharge as the cervix changes.
- Mucus plug: The barrier of mucus that seals the cervix during pregnancy.
- Braxton Hicks contractions: Irregular “practice” contractions that don’t open the cervix.
- Lightening (dropping): The baby settling lower into the pelvis before labor.
- Precipitous labor: Labor and delivery completed in roughly three hours or less.
- Augmentation: Using medication (typically oxytocin) to strengthen contractions that have slowed.
Key Takeaways
- Labor has three core stages — cervical dilation, pushing and birth, and placenta delivery — plus an often-overlooked fourth stage covering the first hours of recovery.
- Stage 1 is the longest and is split into early labor, active labor, and transition, each with distinct dilation ranges and contraction patterns.
- True labor intensifies steadily regardless of activity; Braxton Hicks contractions are irregular and often ease with rest or movement.
- Specific clinical thresholds define “prolonged” labor at each stage, which helps your care team know when intervention may be needed.
- Pain relief ranges from breathing techniques and water immersion to epidurals, nitrous oxide, and, rarely, general anesthesia — there’s no single right choice.
- Not every birth follows the vaginal-delivery script; induction, C-sections, and VBAC all still map onto the same general staged process, with some steps shortened or skipped.
Comparison Table: The Stages of Labor at a Glance
| Stage | What Happens | Typical Duration | Key Signs |
|---|---|---|---|
| Stage 1: Early labor | Cervix dilates to ~6 cm | Hours to 1–2 days | Mild, irregular contractions; bloody show |
| Stage 1: Active labor | Cervix dilates 6–10 cm | 4–8 hours | Strong, regular contractions every 3–5 min |
| Stage 1: Transition | Final dilation to 10 cm | 15 min–2 hours | Intense contractions, nausea, urge to push |
| Stage 2: Pushing/birth | Baby moves through birth canal and is born | Minutes to a few hours | Crowning, delivery of baby |
| Stage 3: Placenta delivery | Placenta separates and delivers | 5–30 minutes | Mild contractions resume |
| Stage 4: Immediate recovery | Body stabilizes, bonding begins | 1–3 hours | Uterine contraction, vital sign monitoring |
FAQ
1. How can I tell true labor from Braxton Hicks contractions?
True labor contractions get progressively stronger, longer, and closer together no matter what you do, and they cause real cervical change. Braxton Hicks contractions are irregular, often ease with rest, water, or movement, and don’t open the cervix.
2. How long does the first stage of labor usually last?
The first stage is typically the longest, lasting 12 to 19 hours total for a first birth, though it’s often shorter for subsequent births. It includes early labor, active labor, and transition.
3. What’s the difference between dilation and effacement?
Dilation measures how open the cervix is, from 0 to 10 centimeters. Effacement measures how thin the cervix has become, from 0% to 100%. Both typically need to be complete before you push.
4. Can my water break before contractions start?
Yes. Some people’s membranes rupture before regular contractions begin, while others don’t experience it until well into active labor or sometimes not until a provider breaks the water manually.
5. Is nausea normal during labor?
Yes, especially during transition, when hormonal shifts and intense contractions commonly cause nausea, chills, or shaking. It usually resolves once you move into the pushing stage.
6. How many centimeters dilated do I need to be before pushing?
Generally you need to reach full dilation — 10 centimeters — before pushing. Pushing earlier can cause the cervix to swell and may slow delivery, so providers usually ask you to wait or use breathing techniques until you’re fully dilated.
7. What is precipitous (rapid) labor?
Precipitous labor describes a labor and delivery that progresses through active labor, birth, and placenta delivery in roughly three to five hours total, essentially skipping a long early phase.
8. How long does it take to deliver the placenta?
The placenta is usually delivered within 5 to 30 minutes after the baby is born. Providers consider it abnormal, and may intervene, if it takes longer than 30 minutes.
9. What is the “fourth stage” of labor?
It refers to the first one to three hours after the placenta is delivered, when your uterus continues contracting, vital signs are monitored closely, and many people experience their first skin-to-skin contact with the baby.
10. When should I go to the hospital?
Common guidance is the “5-1-1 rule”: contractions about five minutes apart, lasting about a minute each, for at least an hour. You should also go in right away if your water breaks, you have heavy bleeding, or you notice a significant drop in fetal movement.

11. Can labor stop and start again?
Yes, particularly during early labor, which can stall, pause, or restart over hours or even days before settling into a consistent active pattern.
12. Does walking help labor progress?
Movement and upright positions are often encouraged because gravity and pelvic mobility can support the baby’s descent, though walking alone doesn’t guarantee faster progress for everyone.
13. What if my labor isn’t progressing?
If dilation stalls beyond specific clinical time thresholds, your provider may suggest position changes, breaking your water, oxytocin augmentation to strengthen contractions, or a C-section if the baby shows signs of distress or labor truly fails to progress.
14. Can I eat during labor?
Many providers allow light eating and drinking during early labor but may restrict you to clear liquids once you’re in active labor or if a C-section becomes more likely, since having food in your stomach can complicate anesthesia.
15. Will I definitely need an episiotomy or get a vaginal tear?
Not necessarily. Many people deliver without either, but minor tears are common and are typically repaired with stitches shortly after delivery in stage 3.