How to Calculate Ovulation With an Irregular Cycle Guide? Learn how to calculate ovulation with an irregular cycle using tracking methods, ovulation tests, and fertility signs to improve your chances of conception. If your period shows up whenever it feels like it, figuring out when you ovulate can feel like guesswork. Most ovulation advice assumes a tidy 28-day cycle — but if yours swings between 24 and 40 days, that math falls apart fast.
The good news: you can still pinpoint your fertile window with an irregular cycle. It just takes a different approach than the standard “day 14” rule — one that uses your own cycle history instead of an average. Here’s how to calculate ovulation with an irregular cycle, plus the tracking methods that work best when the calendar alone isn’t enough.
What Counts as an Irregular Menstrual Cycle?
A “regular” cycle isn’t a single number — it’s a range. Most cycles fall somewhere between 24 and 38 days, and a couple of days of natural variation from month to month is normal.
Your cycle is generally considered irregular if:
- Your cycle length is shorter than 21 days or longer than 35 days
- The gap between your shortest and longest cycle is more than 7–9 days
- You miss three or more periods in a row
- Your cycle length changes noticeably and unpredictably month to month
If any of these sound familiar, the standard “count back 14 days” trick won’t give you a reliable fertile window — but a few adjustments to how you calculate, plus the right tracking tools, can still get you there.
Why Irregular Cycles Make Ovulation Harder to Predict
The Three Phases of Your Cycle
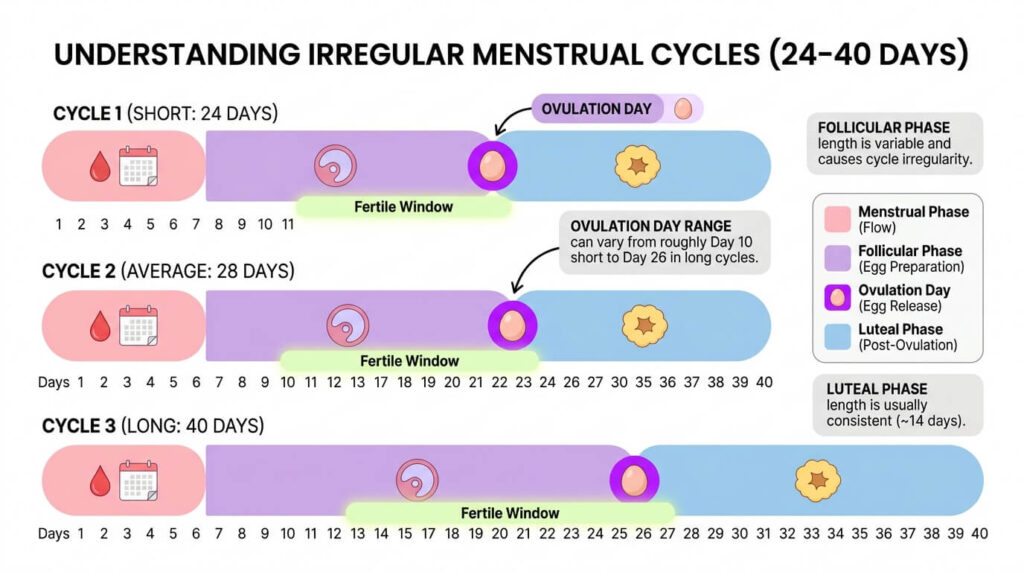
Every cycle moves through three phases, and irregularity almost always comes from variation in the first one:
- Follicular phase — starts on day one of your period. Rising estrogen thickens your uterine lining while follicles in your ovaries mature. This phase is the one that stretches or shrinks the most, which is why total cycle length varies.
- Ovulation — a surge in luteinizing hormone (LH) triggers the release of a mature egg, usually over a 24-hour window.
- Luteal phase — the time between ovulation and your next period. Unlike the follicular phase, this phase is fairly consistent in length (commonly 12–14 days) even when the rest of your cycle isn’t.
That last point matters: because the luteal phase is the stable part of an irregular cycle, tracking methods that detect ovulation directly (rather than counting days from your last period) tend to be far more useful than calendar guesswork alone.
Anovulatory Cycles: When You Bleed But Don’t Ovulate
Here’s something most calculator-style articles skip entirely: having a period doesn’t always mean you ovulated. In an anovulatory cycle, estrogen rises but the egg-releasing LH surge never happens, so progesterone never follows. The uterine lining still builds up and eventually sheds — but that bleed is technically abnormal uterine bleeding, not a true period.
This is one reason irregular cycles can be so confusing to calculate: you might be working backward from a bleed that wasn’t driven by ovulation at all. It’s also why combining a calculation method with a direct ovulation-detection tool (covered below) matters more for irregular cycles than for regular ones.
How to Calculate Ovulation With an Irregular Cycle (Calendar Method)
If you want a starting estimate before adding test strips or temperature charts, clinicians have long used a version of the calendar rhythm method adapted for variable cycles. Instead of using one “average” cycle length, it uses your shortest and longest cycles from the past several months to bracket your likely fertile window.
Step-by-Step: Using 6 Cycles of Data
Your fertile window runs from the earliest day to the latest day, counted from day one of your most recent period.
Track at least 6 cycles. Note the first day of bleeding (true flow, not spotting) for each one. Six is the minimum for a usable range — more is better.
Identify your shortest and longest cycle lengths from that data.
Calculate the earliest likely fertile day: subtract 18 from your shortest cycle length.
Calculate the latest likely fertile day: subtract 11 from your longest cycle length.
Worked Example
Say your last six cycles were 24, 29, 26, 31, 27, and 28 days.
- Shortest cycle: 24 days → 24 − 18 = day 6
- Longest cycle: 31 days → 31 − 11 = day 20
Your estimated fertile window is day 6 through day 20 of your current cycle — a 15-day span. That’s wider than the 5-day window a regular-cycle calculator would give you, which is exactly why this method should be treated as a starting estimate, not a precise prediction. The more your cycle length varies, the wider — and less precise — this window gets.
This is the point where most calendar-only advice stops. For irregular cycles specifically, it’s worth pairing this estimate with a method that detects ovulation as it happens.
Beyond the Calendar: Tracking Methods That Work for Irregular Cycles
Ovulation Predictor Kits (OPKs)
OPKs detect the LH surge in urine that precedes ovulation by about 24–36 hours. With a regular cycle, you’d start testing around day 10. With an irregular one, that starting point isn’t reliable — so testing daily, starting a few days after your period ends, is the practical workaround. It’s more strips, but it’s the most direct way to catch the surge without knowing in advance when it’ll happen.
Basal Body Temperature (BBT)
Your basal temperature rises slightly (roughly 0.4–1°F) right after ovulation. Taken first thing every morning with a sensitive BBT thermometer and logged over a few months, this builds a personal pattern — even if that pattern doesn’t follow a fixed day count. The trade-off: BBT confirms ovulation after it’s already happened, so it’s better for understanding your pattern over time than for catching a fertile window in real time.

Cervical Mucus Monitoring
In the days before ovulation, cervical mucus typically becomes clear, stretchy, and slippery — often compared to raw egg white. Checking daily (with clean fingers, toilet paper, or underwear) costs nothing and works regardless of cycle length, making it one of the more practical tools for irregular cycles specifically.
Which Method Should You Use?
| Method | Best for | Limitation |
|---|---|---|
| Calendar (shortest/longest) | A rough starting estimate | Wide window; less useful the more irregular the cycle |
| OPK (daily testing) | Catching the fertile window in real time | Cost of daily strips; still needs daily testing without a predictable start day |
| BBT charting | Confirming ovulation happened, spotting long-term patterns | Tells you after the fact, not in advance |
| Cervical mucus | Free, immediate, works at any cycle length | Takes practice to read accurately |

For irregular cycles, combining two methods — most commonly daily OPKs with cervical mucus checks — tends to give a more complete picture than relying on any single one. A period-tracking app can help log all three data points (cycle day, test result, mucus changes) in one place, which makes patterns easier to spot over several months.
Common Causes of Irregular Ovulation
Irregular cycles are common and usually explainable. A few of the most frequent causes:
- Polycystic ovary syndrome (PCOS): the most common cause of irregular ovulation, affecting roughly 1 in 10 women of reproductive age. [Flag: cite current prevalence figure from WHO or a similar source.] Immature follicles fail to release eggs consistently.
- Thyroid or pituitary disorders: these glands regulate the hormones driving your cycle, so dysfunction here can throw ovulation off.
- Lifestyle factors: significant stress, rapid weight change, intense exercise, or breastfeeding can all disrupt the follicular phase.
- Life stage: irregular cycles are common in the first year or two after periods start, and again during perimenopause.
Most of these causes are manageable or treatable — irregular cycles are a signal to investigate, not a verdict on fertility.
When to See a Doctor
It’s worth talking to a healthcare provider if:
- Your cycles are consistently shorter than 21 days or longer than 35 days
- You miss three or more periods in a row without being pregnant
- Your cycle length swings by more than 7–9 days between months
- You’re trying to conceive and have tracked for several months without identifying a clear pattern
A doctor can run bloodwork or an ultrasound to identify an underlying cause and discuss options — including ovulation-inducing medication if needed.
Frequently Asked Questions
Can you get pregnant with an irregular period?
Yes. Irregular doesn’t mean absent — if you’re ovulating at all, even unpredictably, pregnancy is possible. It simply takes more tracking effort to catch the fertile window.
How do I know if I’m ovulating if my periods are irregular?
A bleed alone doesn’t confirm ovulation, since anovulatory cycles can also cause bleeding. Daily OPK testing, BBT tracking, or cervical mucus changes are more reliable confirmation than the calendar alone.
What’s considered an irregular menstrual cycle?
Generally, cycles shorter than 21 days or longer than 35 days, or cycle lengths that vary by more than 7–9 days from month to month.

Can ovulation tests be inaccurate with irregular cycles?
The tests themselves are accurate at detecting the LH surge; the difficulty with irregular cycles is timing — not knowing when to start testing. Daily testing solves this but increases cost and effort.
What causes irregular ovulation?
PCOS, thyroid or pituitary issues, significant stress or weight changes, and life stages like adolescence or perimenopause are among the most common causes.
How many days after my period do I ovulate if I’m irregular?
There’s no fixed number — that’s the core challenge of an irregular cycle. The shortest/longest cycle calculation above gives an estimate range, but direct tracking methods (OPK, BBT, mucus) are more reliable than counting days alone.
Key Takeaway
Calculating ovulation with an irregular cycle isn’t about finding the “right” day 14 substitute — it’s about replacing a single fixed number with a range based on your own data, then narrowing that range with a tracking method that detects ovulation directly. Track several cycles, calculate your estimated window using your shortest and longest cycle lengths, and pair that estimate with OPKs, BBT, or cervical mucus monitoring for a clearer picture. If your cycles are consistently erratic, a conversation with your doctor can rule out — or identify and treat — an underlying cause.